Comprehensive and Detailed Explanation:
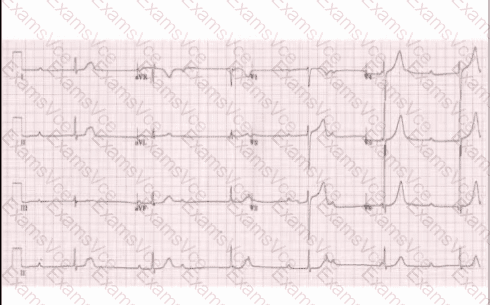
The ECG reveals:
Regular P waves that are not consistently followed by QRS complexes
A dissociation between the atrial (P wave) and ventricular (QRS complex) activity
A slow ventricular rate (~40 bpm) independent of atrial rate
These findings are characteristic of a third-degree (complete) atrioventricular (AV) block, where there is no conduction of atrial impulses to the ventricles. The atria and ventricles beatindependently, and the ventricular rate is maintained by an escape rhythm, often junctional or ventricular in origin.
This correlates with the patient’s symptoms (dizziness, hypotension) and bradycardia, suggesting inadequate cardiac output due to AV dissociation.
Toronto Notes 2023 – Cardiology:
“Third-degree AV block shows complete AV dissociation with independent atrial and ventricular activity. It typically presents with bradycardia and hypotension. Urgent pacing may be required.”
MCCQE1 Objectives (Cardiology > 34-2: Bradyarrhythmias and Conduction Disorders):
“Candidates must identify complete heart block and recognize its clinical urgency.”
Ruling out other options:
A. Sinus bradycardia would show regular P waves with 1:1 P-QRS conduction.
B. First-degree AV block has prolonged PR intervals (>200 ms) but all P waves are conducted.
D. Junctional escape rhythm may present with bradycardia, but P waves would be absent, inverted, or occur after QRS complexes.
E. Mobitz type I (Wenckebach) has progressively lengthening PR intervals before a dropped QRS.
—